
Modern Cementing Technique (MCT) is a standardized and proven procedure for optimal implant fixation in order to improve clinical outcome and achieve long term implant survival.1,2 MCT addresses implant loosening and the objective of MCT is to provide long term implant stability in knee arthroplasty. It is based on scientific data.1-26* findings by Zimmer Biomet27 and evidence-based techniques documented in the Swedish Hip Arthroplasty Register.1,2
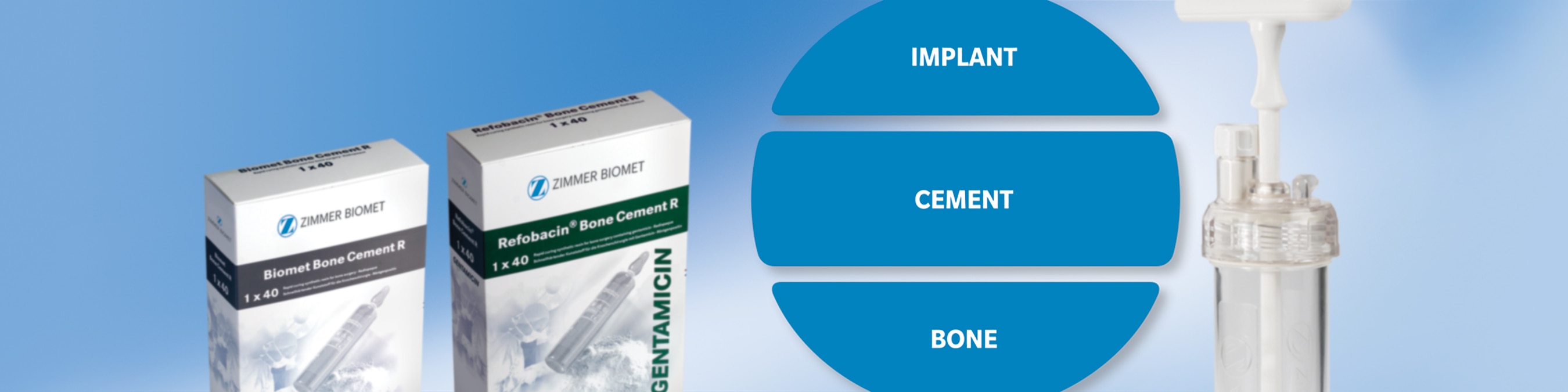
The crucial factors in knee arthroplasty to achieve long term implant stability are to secure a strong bond and optimal interfaces, both between implant-cement and cement-bone.
Zimmer Biomet’s comprehensive assortment of bone cement and products for mixing and delivery, pressurization and bone bed preparation makes for one of the most complete portfolios for Modern Cementing Technique in the market today.